
It rarely starts with collapse.
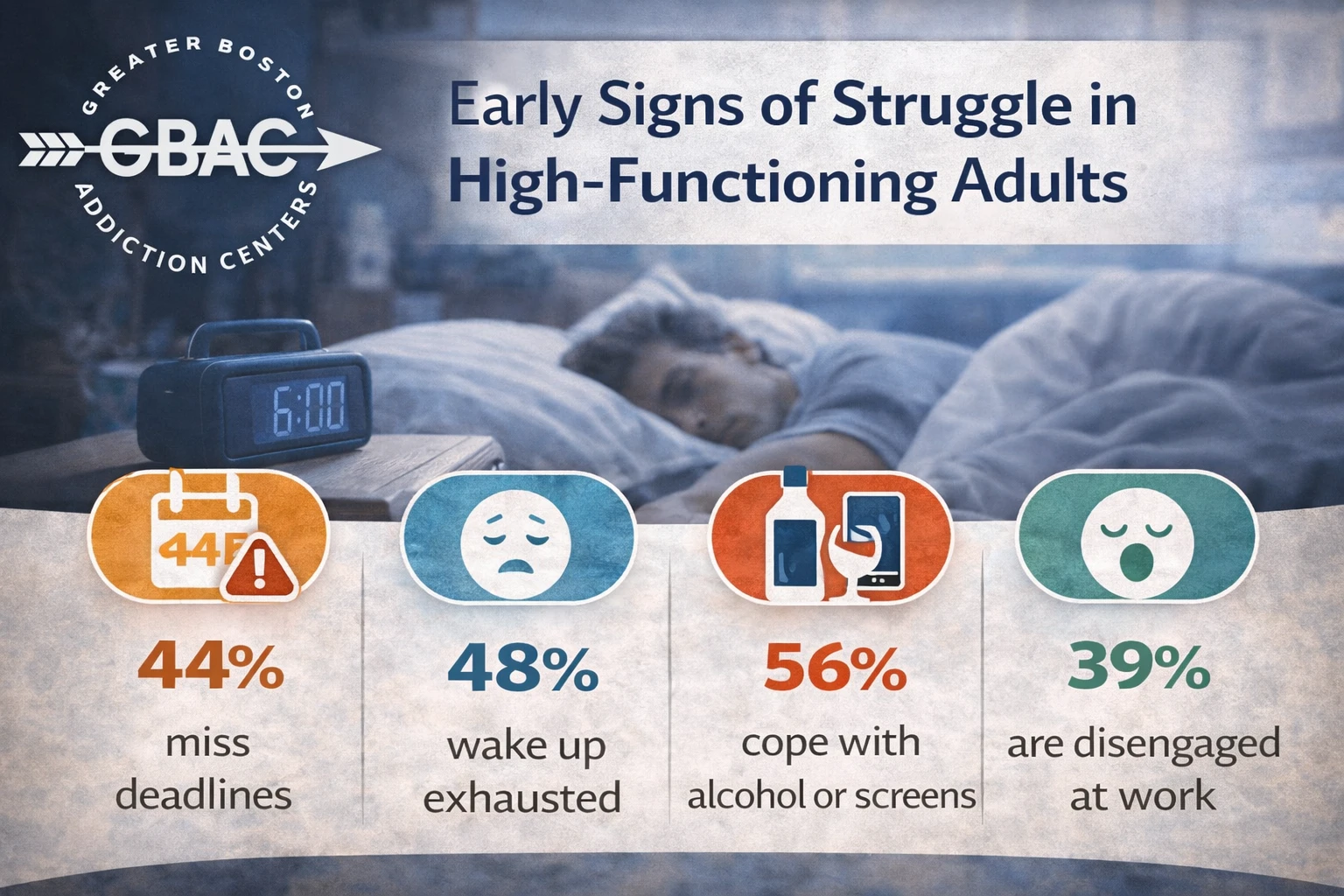
More often, it starts with the small stuff: forgetting a deadline you never would’ve missed, getting short with your kids, sleeping but not feeling rested. Maybe you drink a little more than you used to. Maybe you scroll endlessly at night instead of facing what’s really bothering you. Maybe you wake up tired—not just in your body, but in your bones.
This is what early struggle looks like for high-functioning adults. And this is exactly who we often see in our intensive outpatient program.
They’re not in crisis. Not yet. But something’s shifting. And in the treatment world, we notice that shift long before everything falls apart.
Behind the Mask of “I’m Fine”
Most high-functioning clients are used to wearing the “I’m fine” mask. And the thing is, they’re not lying—not entirely. They are managing. They’re not missing work. They’re not sleeping under bridges. They’re not getting DUIs or overdosing.
But they are unraveling. Quietly.
We notice the subtle signs that family, friends, and even therapists sometimes miss:
- A high performer who suddenly avoids eye contact when talking about weekends
- A parent who laughs a little too hard when joking about “mommy wine time”
- A manager who’s hyper-productive but admits they “can’t turn their brain off at night”
These aren’t dramatic breakdowns. They’re slow leaks. And if no one names them, they just keep growing.
Stress Becomes Strategy
One of the first patterns we see is how stress turns into strategy—but not the good kind. In our IOP groups, clients often talk about how what used to be an occasional crutch is now a default:
- “I used to drink on weekends. Now it’s every night.”
- “I thought I was just unwinding. But I don’t know how to relax without it anymore.”
- “It’s not bad… it’s just constant.”
That’s how dependence starts—not with disaster, but with repetition. And for high-functioning people, this repetition is usually disguised as routine.
It doesn’t look like addiction from the outside. It looks like self-care. But inside, it feels like erosion.
Shame Hides in Professionalism
Clients in our intensive outpatient program often come in with impressive titles and full calendars. Doctors. Lawyers. Parents. Tech leads. Educators.
They’re articulate, organized, and polite. But beneath that, they’re terrified someone will find out they’re struggling. That their carefully curated life is held together with caffeine, cocktails, and white-knuckled willpower.
Shame doesn’t always scream. Sometimes it smiles.
One client once told us, “Everyone thinks I’m the strong one. I don’t know how to tell them I feel like I’m faking it.”
That’s the kind of honesty we hear—not on day one, maybe—but it comes. And when it does, it opens the door to real recovery.
They Don’t Want Labels. They Want Language.
Most high-functioning clients don’t want to be told they’re addicts. They don’t even want to be told they have a “problem.” What they do want is to understand what’s happening beneath the surface.
We give them language for that:
- Emotional exhaustion
- Identity distortion
- Quiet coping
- Internalized performance pressure
The truth is, people don’t need to be pathologized to be helped. They need clarity. And space to explore what they’re feeling without fear of judgment.
That’s one of the core values of our intensive outpatient program—to offer structure and safety without stripping away dignity.
Therapy Isn’t New—But This Kind Is
By the time many clients reach IOP, they’ve tried therapy before. Talk therapy. CBT. Coaching. Even journaling or mindfulness.
But what we hear a lot is this: “I knew what to do, but I couldn’t make myself do it.”
That’s because individual therapy often happens in a vacuum. You go once a week, vent, and try to hold onto a few insights while the rest of life keeps pulling you under.
In contrast, IOP offers:
- Multiple sessions per week (group + individual)
- Peers who reflect your experience back to you
- Real-time accountability and progress
- A rhythm that rewires—not just reviews—behavior
It’s less about coping hacks and more about rewiring your relationship to stress, self-worth, and substances.
And when needed, we sometimes guide clients toward deeper stabilization in residential treatment—especially if emotional overwhelm becomes unmanageable. But often, outpatient care is the perfect place to begin.
What We Notice Before Crisis Happens
Here are some of the specific patterns we watch for—and intervene on—early:
- Perfectionism masking burnout: The harder someone pushes themselves, the more hollow they often feel.
- Sarcasm shielding sadness: Humor is safe. But when it becomes the only way someone shares truth, we know there’s pain underneath.
- High compliance with little connection: Doing the “work” without feeling the work means someone’s checked out emotionally.
- Eroding self-trust: When someone keeps promising themselves they’ll cut back… and doesn’t.
These signs aren’t failures. They’re flags.
And we’d rather someone walk in with those early flags than wait for everything to collapse.
Quiet Doesn’t Mean Small
One of the most profound things we see in IOP is that the quietest breakthroughs often lead to the biggest shifts.
- Someone finally admits: “I don’t know how to feel my feelings.”
- Another says: “I think I’m scared of being okay, because I don’t know what that would feel like.”
These aren’t dramatic therapy moments. But they’re real. And they matter.
Because real change often begins when someone stops trying to explain themselves—and just tells the truth.
Dorchester, Massachusetts is home to one of our recent IOP clients who said something that stuck with us: “I didn’t know how much I was suffering until I stopped pretending I wasn’t.” That’s why early support matters. That’s why watching quietly isn’t enough. That’s why we speak up—even before crisis.
Frequently Asked Questions
What is an intensive outpatient program (IOP)?
An IOP is a structured treatment format that includes multiple weekly therapy sessions—individual, group, and sometimes family—while allowing participants to continue daily responsibilities at home or work.
Is IOP only for people with substance issues?
Not at all. While many clients do use substances, we also work with those navigating stress, emotional burnout, trauma, and anxiety—even if substances aren’t involved.
Do I have to call myself an addict to be eligible?
Absolutely not. Many of our clients never use that label. If something isn’t working, and you want help—that’s enough.
How long does an IOP last?
Program lengths vary, but most clients participate for 6 to 12 weeks. We tailor the timeline based on your needs and progress.
Can I keep working while doing an IOP?
Yes. Most IOPs are scheduled around typical work hours, with morning or evening options. Flexibility is part of the model.
What happens if I need more support than IOP?
If we notice signs that deeper care is needed, we’ll walk you through other options, like residential care, without judgment or pressure.
West Roxbury, Massachusetts is where one client told us they felt like the “most put-together broken person” they knew. They weren’t in crisis when they came to us. They just didn’t want to get there.
And that was reason enough to begin.
Call (877) 920-6583 to learn more about our intensive outpatient program in Boston, Massachusetts.